Epidemiology
Global Information
The occurrence of pterygium was discovered to be 10.2% worldwide, with highest
possible prevalence in reduced altitude regions.
Increased incidence of pterygium is noted in the tropics as well as in an equatorial
zone in between 30 ° north as well as southern latitudes, Liu et al, 2013.
Higher occurrence is related to persistent sunlight exposure (ultraviolet light), older
age, male sex, as well as exterior activity, Liu et alia, 2013.
Regional Info (Latin America)
One study amongst a Latino population in Tucson Arizona, USA found the frequency
of pterygium to be 16%, West et al, 2009.
A hospital-based research in Lima, Peru, reported the prevalence of pterygium to be
31%, with a considerable rise in occurrence with enhancing age, Rojas et al, 1986.
In a population-based example in Botucatu City, Sao Paulo State, Brazil, the reported
occurrence was 8.12%, impacting primarily 40-50 year old men, Shiratori et al, 2010.
Differential diagnosis
Pseudopterygium
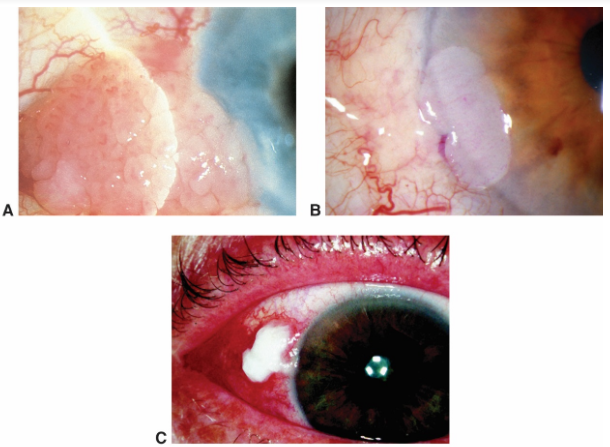
neoplasia. A. Papilliform. B. Gelatinous. C. Leukoplakic
Conjunctival and corneal intraepithelial tumor (CIN)
Interpretation
Pterygium originates from the Greek word meaning wing, pterygos.
Pterygium is a triangular fibrovascular growth that expands from the conjunctiva
towards the cornea.
It is much more typical in the interpalpebral fissure area as well as might occur
occasionasally or temporally or both. The nasal location is much more typical.
Although the pathophysiology is not clearly comprehended, ultraviolet (UV) light is
recognized as one of the most essential danger elements.
UV light forms complimentary radicals that cause damages in DNA, RNA, and also
the extra celluar matrix of cells.
Ultraviolet-B (UVB) causes expression of cytokines as well as growth factors in
pterygial epithelial cells.
Polymorphisms of the DNA break repair fixing genetics Ku70 have actually been
connected with hereditary predisposition to pterygia growth.
Increased levels of T-cells as well as inflammatory markers have actually additionally
been kept in mind in pterygial cells contrasted to regular conjunctival cells.
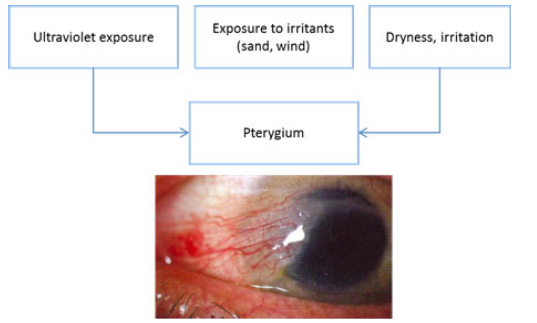
Risk Elements
Ultraviolet direct exposure solitary most substantial risk element.
Exposure to irritants (dirt, sand, wind).
Inflammation.
Dry eye surface.
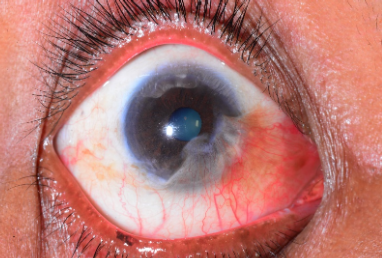
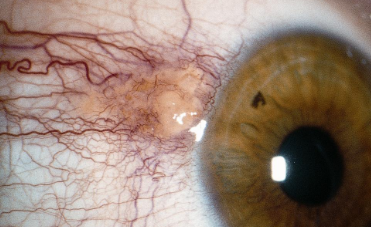
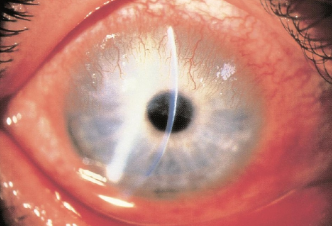
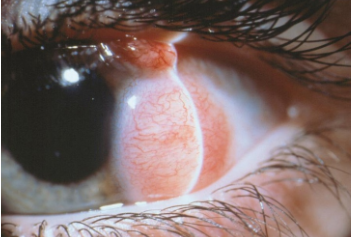
Symptoms
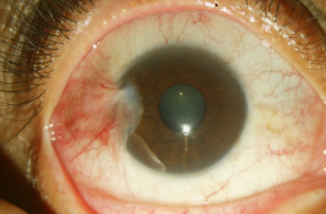
Slit-lamp image of a pterygium.
Wedge-shaped, transparent membrane layer with apex prolonging onto cornea.
White to pink in color, depending upon vascularity.
Vascular straightening towards the progressing head of the pterygium.
Stocker line: iron line on cornea at leading side of pterygium.
Regular or irregular astigmatism
Degenerative changes such as cystic changes.
May be asymptomatic.
Redness.
Irritation.
Decreased vision.
Medical diagnosis
Diagnosis is made scientifically based upon slit-lamp evaluation and also typical
appearance of the lesion.
Management
excision.

Prevention
Wearing eye protection, sunglasses, safety glasses, and/or an overflowed that is
suggested when one is exposed to sunlight or dirt. Sunglasses that obstruct 99%–
100% of both UVA as well as UVB rays are preferred.
Medical Monitoring.
Small pterygia without aesthetic impairment can be dealt with symptomatically with
artificial tears as well as eye lubricants.
Clinical therapy (man-made tears and lubricants) does not reduce progression or
cause regression of pterygia.
In patients with irritative signs and symptoms, preservative-free man-made tears are
suggested for moderate inflammation as well as topical steroids are advised for
modest inflammation.
Monitoring pterygia at 6– 12 months is practical.
Surgical Monitoring
Surgical removal is taken into consideration for the following problems:
Decrease in aesthetic acuity because of astigmatism or infringement onto aesthetic
axis.
A cosmetically significant pterygium.
When it interferes with contact lens wear.
Symptomatic degenerative changes like cystic changes.
Restriction of extraocular motions.
Surgical techniques consist of the following:
Simple excision without transplant, also known as bare sclera is associated with a
higher recurrence rate as well as for this reason it has actually been supplemented
with conjunctival transplantation.
Adjuvant therapies including mitomycin C (MMC), 5-fluorouracil (5-FU), ethanol,
irradiation, and also anti-angiogenic agents to name a few, are utilized to reduce
recurrence rate, however there is insufficient evidence that it is superior, Kaufman et
al, 2013.
The perfect treatment recommended entails excision of pterygium with conjunctival
autograft (CAG) supplements. Conversely, if there is insufficient conjunctiva, then
amniotic membrane transplant (AMT) might be glued or sutured right into place.
Treatments utilizing fibrin glue take around half the time as surgical treatments using
stitches as well as patients usually report much less postoperative surgical pain and
also discomfort, Marticorena, Joaquin et al, 2006. Nevertheless, fibrin glue is much
more costly and also can be challenging to acquire in some countries. The glue is a
blood-derived product as well as carries the danger nevertheless minimal of viral and
also prion disease.
An additional approach is autoblood graft fixation, a technique also known as stitch-
and glue-free autologous graft. This strategy affixes the graft right into place with the
patient’s own blood, doing away with the concern of disease transmission.
Postoperative Monitoring
Patch/shield overnight.
Drops: Steroid antibiotic combination 4 times a day for 1 month.
Difficulties of Pterygium Surgical Treatment
Intraoperative:
Buttonhole of the conjunctival autograft.
Injury to extraocular muscles.
Postoperative:
Graft slippage.
Graft retraction.
Donor site granuloma formation.
Long-term complications:
The most common difficulty is recurrence after removal. The recurrence rate is as
high as 50% within 4 months and also 97% recurrence rate within one year without
autograft or amniotic membrane transplant, Hirst LW, 2003. The recurrence rate is
higher with fleshy, nontranslucent pterygia as well as increased postoperative
inflammation. The recurrence rate is decreased to 5%– 10% with conjunctival
flap/graft supplements.
Other complications include corneal scarring, corneal perforation, strabismus,
nonhealing problem specifically with mitomycin C, scleral melt as well as scleral
dellen, Kaufman, SC et al, 2013.
CASE STUDY
History of Existing Illness
A 45-year-old patient, Della, presented with hyperemia, foreign body sensation, and also
irritation in her right eye without improvement after man-made tears. Her family history is
significant for diabetes. Eyelids of the right eye were within normal limits. The best eye had
moderate conjunctival hyperemia as well as a 2– 3 mm temporal pterygium without
involvement of the papillary area. Eye examination of the left eye was normal.
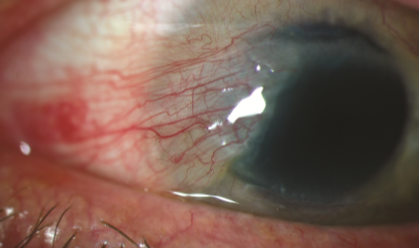
Treatment
Surgical Procdure of pterygium plus conjunctival autograft in right eye. One week after
surgery, there is mild conjunctival hyperemia and chemosis with complete resection of the
pterygium.

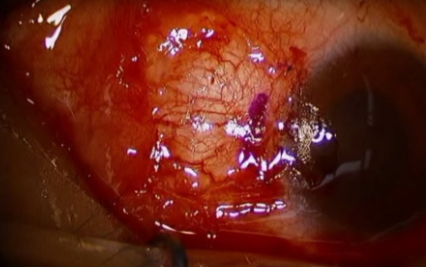
One week after surgery of the pterygium and placement of temporal conjunctival autograft.